

Abstract
Background: Osteonecrosis and osteopenia frequently complicate acute lymphoblastic leukemia (ALL) therapy. Interventions which reduce these bony toxicities without impairing the anti-leukemic efficacy of therapy are lacking. Case reports suggest that bisphosphonates may reduce the pain associated with osteonecrosis; however, it is unclear if they are effective in preventing or reducing the progression of osteonecrosis or modifying bone density loss during therapy. Their impact on the anti-leukemic efficacy of therapy is also unknown.
Methods: We tested the efficacy of the bisphosphonate zoledronic acid (ZA) in the murine model of osteonecrosis. Four-week-old Balb/c mice were treated with dexamethasone (2mg/L in drinking water) and PEGylated-asparaginase [1200IU/kg intraperitoneal (IP) weekly] for 6 weeks. To test whether ZA could prevent osteonecrosis, mice received ZA 100ug/kg IP weekly starting with therapy initiation (early zoledronic acid group, receiving 6 total doses). To test whether ZA could prevent the progression of osteonecrosis, ZA administration was delayed until the fourth week of therapy (late zoledronic acid group, receiving 2 total doses) after osteonecrosis processes have already begun. All mice were humanly euthanized at 10 weeks post-natal. At the end of the 6 week therapy, osteonecrosis was assessed histologically at the distal femur, while bone density and quality measurements were obtained from the proximal tibia using the Siemeons Inveon uCT system.
To test the impact of zoledronic acid on the anti-leukemic efficacy of therapy, nine-week-old B6 mice were injected with 2000 Arf-/- Bcr/Abl+ syngeneic acute lymphoblastic leukemia cells. Mice received three weeks of therapy identical to the osteonecrosis studies (including zoledronic acid randomization), except dexamethasone was increased to 4mg/L in the drinking water. Mice were sacrificed when moribund and leukemia as cause of death was confirmed by peripheral white blood cell count and spleen weight.
Results: Osteonecrosis was reduced in the early zoledronic acid group compared to the control group (12/69 limbs vs. 25/72 limbs, p=0.03). The incidence of osteonecrosis in the late zoledronic acid group (19/56 limbs) was identical to that in the control group (p=1). Both zoledronic acid interventions increased the cortical thickness of the tibia [median 0.12mm in therapy treated controls; 0.18mm in early zoledronic acid group (p=<0.001 vs. control); 0.15mm in late zoledronic acid group (p=<0.001 vs. control)]. Thinner cortical wall thickness was associated with an increased risk of osteonecrosis in univariate analysis (p=0.03) but not in multivariate analysis including treatment arm (p=0.32). Epiphyseal arteriopathy, the preceding vascular lesion in osteonecrosis, was less common in early zoledronic acid mice vs. controls (15/60 vs. 28/51, p=0.002). Late zoledronic acid administration resulted in a similar rate of arteriopathy (22/47) compared to controls (p=0.55). There was no difference in the incidence of asparaginase plasma concentrations <1u/mL (p=0.25) or in plasma dexamethasone levels (p=0.67) in mice receiving ZA vs. control treated mice.
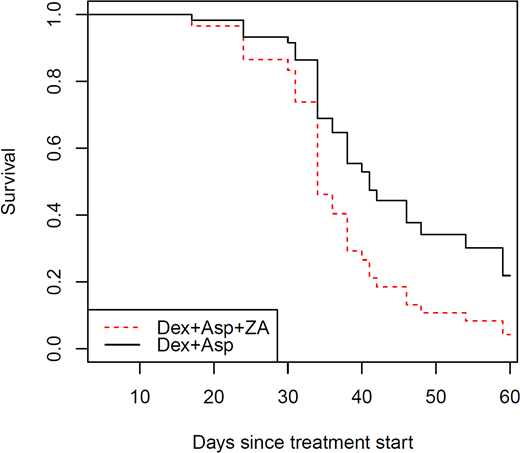
Because early zoledronic acid administration reduced the rate of osteonecrosis and improved bone density, we tested its effect on the anti-leukemic efficacy of therapy. Mice that received zoledronic acid and chemotherapy had a shorter survival than mice receiving chemotherapy alone (mean 36 vs. 41.6 days, log-rank p=0.046, Figure 1).
Conclusion: Zoledronic acid administration early in acute lymphoblastic leukemia therapy reduces osteonecrosis and osteopenia. Zoledronic acid is ineffective in reducing osteonecrosis when given later in therapy. However, the use of zoledronic acid impairs the combined anti-leukemic efficacy of dexamethasone and asparaginase. Further studies are underway to understand this relationship.
Relling:Shire Pharmaceuticals: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal